The Role of Skin Remodeling in Healing Explained
- L Guevara
- 9 hours ago
- 8 min read

Skin remodeling is defined as the final phase of wound healing, during which the body reorganizes collagen fibers and rebuilds the extracellular matrix (ECM) to restore skin strength and function. This phase begins 2–3 weeks after injury and can last a year or longer, making it the longest and most complex stage of the skin healing process. The role of skin remodeling in healing goes far beyond closing a wound. It determines whether you end up with a flat, faded scar or a thick, raised one, and it directly shapes the long-term appearance and resilience of your skin. Understanding what drives this process gives you real leverage over your healing outcomes.
What happens during the skin remodeling phase of healing?
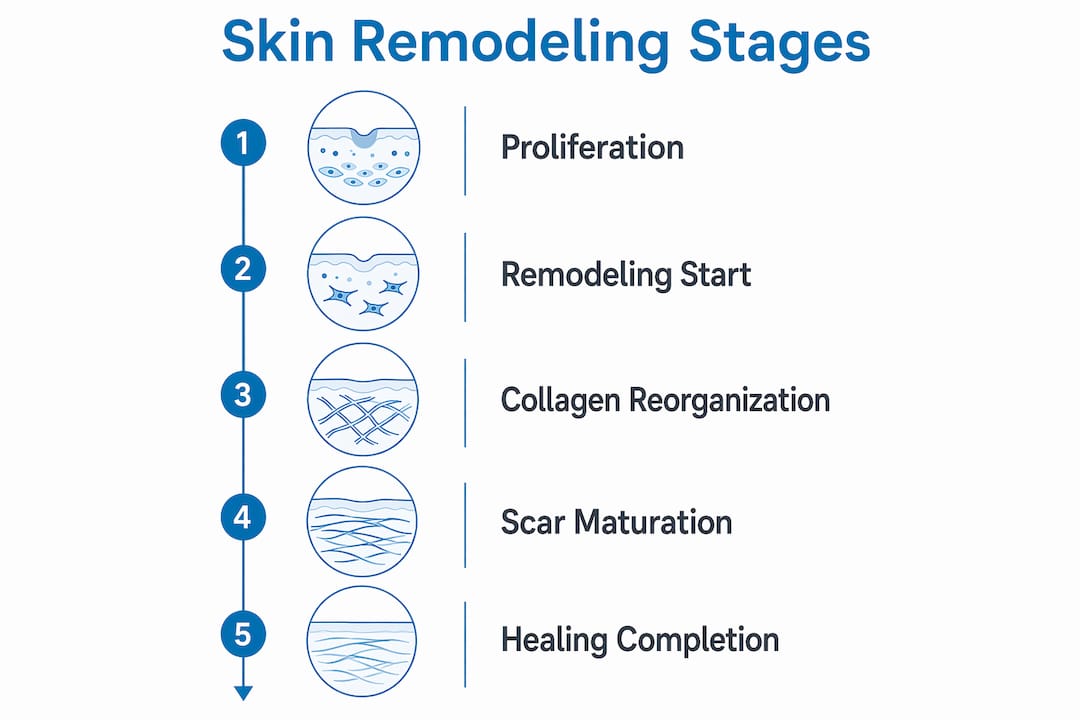
Remodeling begins when the proliferation phase winds down, roughly 2–3 weeks post-injury. During proliferation, myofibroblasts contract the wound by physically pulling its edges together, setting the stage for the structural refinement that follows. Once contraction is complete, the body shifts its focus from building new tissue to improving the quality of what it built.

The most critical event in this phase is a collagen swap. The body replaces weaker Type III collagen, laid down quickly during proliferation, with stronger Type I collagen. This exchange is controlled by enzymes called matrix metalloproteinases (MMPs), which break down old collagen while fibroblasts deposit new fibers in more organized patterns. Advanced imaging techniques like second-harmonic generation (SHG) microscopy reveal the difference clearly: healthy skin shows a “basket-weave” collagen pattern, while scar tissue shows tightly aligned bundles.
Vascular regression also occurs during remodeling. The dense network of blood vessels formed during proliferation gradually recedes, which is why fresh scars appear red and then fade over months. Tensile strength recovers progressively, reaching approximately 80% by 12 months. That ceiling matters: even fully remodeled skin never quite matches original tissue.
Proliferation ends. Myofibroblasts complete wound contraction and undergo apoptosis.
Collagen exchange begins. Type III collagen is degraded and replaced with Type I.
MMPs regulate turnover. Enzymes balance ECM breakdown and new fiber deposition.
Vasculature recedes. Excess blood vessels regress, reducing redness.
Tensile strength builds. Skin regains mechanical integrity over months to a year.
Pro Tip: Keeping a healing wound moisturized and protected from UV exposure during the remodeling phase supports better collagen organization and reduces the risk of hyperpigmented or thickened scars.
How does skin remodeling influence scar formation and regeneration?
Not all healing leads to scarring. The outcome depends heavily on which fibroblast subpopulations dominate the wound environment. Research published in Science shows that Engrailed-1 positive fibroblasts drive scar formation, while Engrailed-1 negative fibroblasts promote regenerative healing that restores hair follicles and glands.
What activates Engrailed-1? Mechanical tension. When a wound is under physical stress, fibroblasts sense that tension through a process called mechanotransduction and activate scarring pathways. Blocking YAP signaling, a key mechanotransduction mediator, prevents Engrailed-1 activation and redirects healing toward regeneration. This finding is one of the most significant shifts in wound biology in recent years.
Scarless healing is not a matter of luck. It is a matter of which fibroblast population wins. Mechanical tension tips the balance toward scarring, and targeting that tension at the molecular level can redirect the outcome entirely. The implication for aesthetic medicine is profound: controlling the wound environment during remodeling is as important as any topical treatment applied after the fact.
Several factors determine whether repair or regeneration dominates:
Wound size and depth. Larger, deeper wounds recruit more Engrailed-1 positive fibroblasts.
Mechanical tension. High-tension areas like the chest and shoulders scar more aggressively.
Skin appendages. Scars lack hair follicles and sweat glands because regenerative fibroblasts were not dominant.
Molecular targets. TGF-β/Smad and FAK signaling pathways modulate scar suppression and are active areas of therapeutic research.
Wound closure method. Primary intention closure (sutured wounds) produces far less scarring than secondary intention (wounds left to heal open).
Understanding why scars change color over time connects directly to these remodeling events. Redness fades as vasculature recedes. Pigmentation shifts as keratinocytes and melanocytes normalize. Both are signs that remodeling is progressing.
What roles do the extracellular matrix and growth factors play in skin remodeling?
The ECM is not passive scaffolding. It is a dynamic reservoir for growth factors and cytokines that regulate fibroblast activity, immune cell behavior, and tissue organization throughout the remodeling phase. When ECM components bind to cellular receptors called integrins, they trigger signaling cascades that tell fibroblasts when to produce collagen and when to stop.
Three growth factors drive most of the remodeling activity:
Growth Factor | Primary Role | Consequence of Imbalance |
TGF-β | Stimulates collagen synthesis and fibroblast activation | Excess leads to fibrosis and hypertrophic scars |
PDGF | Recruits fibroblasts and promotes cell proliferation | Deficiency slows remodeling and delays closure |
VEGF | Supports vascular remodeling and tissue oxygenation | Excess causes persistent redness; deficiency impairs healing |
MMP activity is the central regulator of ECM turnover. When MMPs and their inhibitors (TIMPs) stay in balance, the ECM remodels cleanly. When that balance breaks, chronic wounds and fibrosis develop. Chronic wounds show persistent inflammation, protease imbalance, and microbial colonization that prevent effective remodeling from ever completing.
Non-healing wounds carry a significant cost. In the United States, non-healing wounds cost approximately $50 billion annually. That figure reflects the clinical and economic weight of failed remodeling at scale.
Pro Tip: Topical treatments containing retinoids or peptides can support MMP regulation and collagen synthesis during the remodeling phase. Pairing them with professional skin therapies amplifies results.
How long does the remodeling phase last?
The remodeling phase begins 2–3 weeks after injury and can extend well beyond a year for deep or complex wounds. Most people underestimate this timeline because the wound looks closed long before remodeling is complete. Visible closure and structural maturity are two very different milestones.
Several factors shape how long remodeling takes and how well it goes:
Wound type and depth. Superficial abrasions remodel in weeks. Deep surgical wounds or burns can take 12–18 months.
Closure method. Primary intention (sutured) wounds remodel faster and with less scarring than secondary intention wounds.
Underlying health conditions. Diabetes and vascular disease impair circulation and growth factor delivery, slowing every phase of healing.
Age. Older skin produces collagen more slowly and with less efficiency, extending the remodeling timeline.
Wound care quality. Consistent moisture, sun protection, and avoiding mechanical stress all support better remodeling outcomes.
A common misconception is that a scar is “done” once it stops feeling tight or itchy. In reality, collagen reorganization continues for months after those sensations fade. Scars often soften, flatten, and lighten significantly between months 6 and 18. Patience is not passive. It is part of the treatment plan.
The connection between stretch mark treatments and remodeling timelines follows the same logic. Stretch marks are a form of dermal scarring, and staged interventions that respect the remodeling timeline produce better results than aggressive early treatment.
How can understanding skin remodeling improve healing and aesthetic outcomes?
Knowing how remodeling works changes how you approach both wound care and aesthetic treatments. The biology gives you a framework for timing decisions, selecting therapies, and setting realistic expectations.
Timing matters for procedures. Non-surgical treatments like microneedling and radiofrequency work by triggering controlled remodeling. Applying them too early in a healing wound disrupts the natural process. Applying them at the right stage amplifies collagen reorganization.
Mechanotransduction is a therapeutic target. Targeting TGF-β/Smad and FAK signaling shows real potential for reducing scar formation. Clinical applications of this research are emerging in both medical and aesthetic settings.
Pre-treatment preparation supports remodeling. Skin that is well-hydrated, nutritionally supported, and free of active inflammation remodels more effectively. Prepping skin before non-surgical treatments is not optional. It is foundational.
Regenerative medicine is advancing fast. Cell therapies targeting fibroblast subpopulations and ECM signaling are moving from laboratory research toward clinical trials. The goal is not just faster healing but genuinely scarless healing.
Scar appearance reflects remodeling quality. A flat, skin-toned scar signals well-organized Type I collagen. A raised, red scar signals ongoing inflammation or excess fibroblast activity. Knowing the difference helps you choose the right intervention at the right time.
Understanding skin rejuvenation through the lens of remodeling biology also reframes what “results” mean. Aesthetic improvement is not separate from healing. It is the visible outcome of remodeling done well.
Key Takeaways
Skin remodeling is the longest phase of wound healing, and its quality, not just its completion, determines both the functional and aesthetic outcome of every injury or procedure.
Point | Details |
Remodeling timeline | The phase starts 2–3 weeks post-injury and can last over a year for complex wounds. |
Collagen quality drives outcomes | Type I collagen replacement of Type III restores tensile strength, reaching roughly 80% of original by 12 months. |
Fibroblast subpopulations decide scarring | Engrailed-1 positive fibroblasts cause scarring; blocking YAP signaling can redirect healing toward regeneration. |
ECM balance is non-negotiable | MMP and TIMP imbalance leads to chronic wounds or fibrosis; growth factors TGF-β, PDGF, and VEGF regulate this balance. |
Timing shapes treatment success | Non-surgical aesthetic procedures work best when applied at the right remodeling stage, not immediately after injury. |
What I’ve learned from watching skin remodel up close
Working in aesthetic skin care, I see the remodeling phase misunderstood more than any other part of healing. Clients come in frustrated that their scar “isn’t going away” at the six-week mark, not realizing that the real work is still happening beneath the surface. The skin is not stalling. It is reorganizing.
What strikes me most about the recent research on Engrailed-1 and mechanotransduction is how much it validates what experienced practitioners have observed for years: wound environment matters as much as wound treatment. A scar on the chest or shoulder almost always looks worse than one on the face, and now we know why. Tension activates the scarring pathway at the cellular level.
The practical takeaway I share with every client is this: the remodeling phase is not a waiting room. It is an active window where the right support, whether topical, procedural, or lifestyle-based, can meaningfully shift the outcome. Scars that look discouraging at two months often look dramatically different at twelve. That is not wishful thinking. That is biology.
I also believe the field is on the edge of something significant with regenerative therapies targeting fibroblast pathways. The idea that we could redirect healing toward true regeneration, with restored follicles and glands, rather than just better-looking scar tissue, is not science fiction anymore. It is the direction the research is pointing, and I find that genuinely exciting.
— Lux
Skin healing support at Luxveritae
Luxveritae offers professional treatments designed to work with your skin’s natural remodeling process, not against it. Whether you are addressing post-procedure recovery, pigmentation changes, or the visible effects of aging on skin structure, the team at Luxveritae builds treatment plans around your skin’s current healing stage.

Specialized services like under-eye lightening treatments address areas where delicate skin remodels slowly and requires precise, calibrated care. Every treatment at Luxveritae is tailored to your skin type, goals, and timeline. Browse the full treatment menu and book a consultation to find out which approach fits where your skin is right now.
FAQ
What is the role of skin remodeling in healing?
Skin remodeling is the final phase of wound healing, during which Type III collagen is replaced with stronger Type I collagen and the extracellular matrix is reorganized to restore tensile strength and skin function. It begins 2–3 weeks after injury and can last over a year.
How long does the skin remodeling phase last?
The remodeling phase typically starts 2–3 weeks post-injury and continues for up to 12–18 months depending on wound depth, closure method, and individual health factors. Tensile strength reaches approximately 80% of original by 12 months.
Why does scar tissue look different from normal skin?
Scar tissue lacks the “basket-weave” collagen pattern of healthy skin and instead shows tightly aligned collagen bundles. It also lacks hair follicles and sweat glands because regenerative fibroblast pathways were not dominant during remodeling.
What factors affect how well skin remodels after injury?
Wound depth, closure method, age, underlying conditions like diabetes, and the quality of ongoing wound care all influence remodeling outcomes. Mechanical tension on the wound site also activates scarring pathways at the cellular level.
Can skin remodeling be improved with treatments?
Yes. Non-surgical procedures like microneedling and radiofrequency stimulate controlled remodeling when applied at the right stage. Topical treatments containing retinoids or peptides support collagen synthesis, and emerging therapies targeting TGF-β/Smad signaling show potential for reducing scar formation.
Recommended